

A new study has revealed that patients living with rosacea, a chronic skin condition affecting individuals with Fitzpatrick skin types I and II and those with photosensitive skin, are at high risk of malignancies and comorbidities. The prevalence of rosacea is ~5.46% in the general population and is more common in individuals >65-years.1,2

Among malignancies, studies included in a 2023 review by Thapa et al report that rosacea was associated with a risk of basal cell carcinoma (41%), squamous cell carcinoma (33%), breast cancer (8%) and melanoma (8%). Furthermore, the condition has been linked to an increased risk of comorbidities including cardiovascular, gastrointestinal, neurologic, psychiatric, and autoimmune diseases. Psychiatric comorbidities such as depression, social phobia, and anxiety have a profound impact on the quality of life of patients.1,2,3
Main phenotypes and characteristics
The main phenotypes of rosacea include:4
- Erythematotelangiectatic: Characterised by flushing and persistent central facial erythema. Redness may also involve the peripheral face, ears, neck and upper chest, but peri-ocular (around the eyes) skin is typically spared.
- Papulopustular: Patients develop papules or pustules in a central facial distribution. In severe cases, these episodes of inflammation can lead to chronic facial oedema.
- Phymatous: Characterised by thickened skin with enlarged pores and irregular surface nodularities. These changes are most commonly found on the nose, but can occur on the ears, chin and forehead. This subtype is more common in men than women.
- Ocular: Characterised by a watery or bloodshot appearance of the eyes, foreign body sensation, burning or stinging. Blepharitis, conjunctivitis, dryness, itching, light sensitivity, blurred vision and telangiectasia of the conjunctiva or eyelids also occur. Chalazia and styes are more common in ocular rosacea than other forms. Because there is no specific test, the diagnosis relies on clinical judgment. Ocular involvement is estimated to occur in 6%-50% of patients living with rosacea and can occur with or without rosacea.
Disease pathogenesis
Rosacea manifests as persistent redness and sensations of itching, burning, or stinging. It is caused by a complex interplay of factors involving skin barrier dysfunction and environmental/genetic triggers. Skin barrier disruption enables bacterial colonisation, and the combination of damaged skin with bacteria, along with antimicrobial peptides, may initiate and activate rosacea.1,3
Cathelicidins, short peptides with antimicrobial effects, play a crucial role in rosacea. The peptide leucine and lysine (LL)-37 has been implicated in erythema and pustule phenotypes. Toll-like receptors induce the serine protease Kallikrein-5, which cleaves LL-37 into pro-inflammatory fragments. This cascade leads to mast cell activation, angiogenic chemokine release, and NOD-like receptor family, pyrin domain-containing 3 inflammasome activation. LL-37 also activates the purinergic 2X7 receptor, contributing to sunlight sensitivity in rosacea.1
Additionally, LL-37 acts as a chemoattractant for mast cells and enhances their antimicrobial properties. Autophagy activation by LL-37 through mammalian target of rapamycin complex 1 and mitogen-activated protein kinase pathways is associated with maintaining cellular homeostasis in response to stressors.1
Transient receptor potential (TRP) channels, essential for ion entry modulation, are implicated in rosacea. Upregulated TRP vanilloid (TRPV) channels, particularly TRPV4, contribute to flushing and stinging phenotypes. TRP ankyrin 1, acting on nociceptive sensors, potentiates inflammatory responses in rosacea.1
Mast cell activation and degranulation are key in rosacea pathogenesis, contributing to disease chronicity. Mast cells respond to various stimuli, including microvesicle particles and toll-like receptor ligands, releasing cytokines, chemokines, and lipid mediators.1
Rosacea triggers
Rosacea exacerbations can be caused by various triggers. Dietary adjustments, including avoiding heat-related (hot drinks), alcohol-related (wine, hard liquor), capsaicin-related (spices, peppers), and cinnamaldehyde-related foods, are often recommended.3
Emerging research suggests an intestine-skin connection, emphasising the importance of fibre intake and probiotics for a healthy intestinal microbiome. Nutrients like omega-3 fatty acids and zinc may offer symptomatic relief, but more research is needed.3
Sun exposure worsens symptoms through various mechanisms, including overexpression of cathelicidin induced by vitamin D. Alcohol and tobacco exacerbate rosacea, with nicotine's angiogenic action triggering symptoms. Face masks exacerbate facial dermatoses, especially in healthcare professionals. Selecting the correct mask type and using it properly are important. Polypropylene masks may cause allergic contact dermatitis. Selecting a fabric masks with a low thread count, smooth surface, light colours, and no metal parts are recommended.3
Managing rosacea is challenging
The management of rosacea is challenging. Management involves various treatment modalities such as skin care, systemic and topical therapies, laser and light-based treatments, as well as invasive methods (eg microneedling). According to the latest guideline by the global Rosacea Consensus panel, the effective management of rosacea involves a multifaceted approach. General skincare education, the use of sunscreen (SPF 30+) and moisturisers, as well as gentle cleansers, and trigger avoidance form the core of management. For primary cutaneous features like erythema, papules/pustules, telangiectasia, and phyma, a phenotype-led treatment algorithm is recommended (see Table 1).5
Table 1: A phenotype‐led treatment algorithm for the cutaneous features of rosacea5
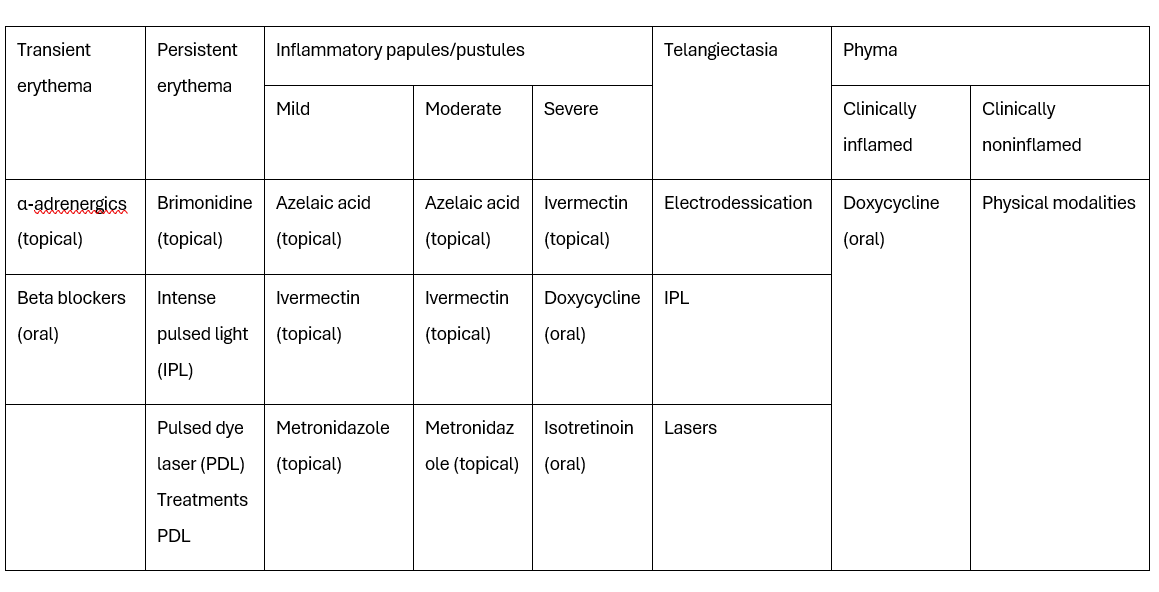
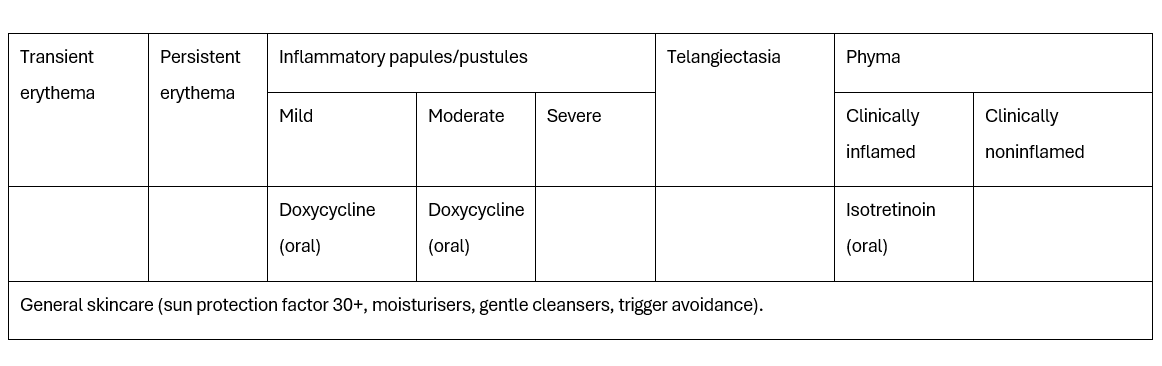
The severity of inflammatory papules/pustules guides treatment decisions, while phyma treatment depends on clinical status. Combination therapy is recommended for multiple features if first-line treatment fails. Moderate and severe cases may require a combination of general skincare, physical modalities, and pharmaceutical agents.
Severe ocular symptoms uncontrolled by lid hygiene may necessitate ophthalmologist involvement. General eye care, including ultraviolet-coated sunglasses and proper lid hygiene, is crucial. Ocular treatments, especially topical medications, are considered to have additive effects. When ocular rosacea coexists with cutaneous features, an optimised combination of therapies addressing both aspects is deemed ideal. Overall, comprehensive patient education and individualised treatment plans are crucial in rosacea management.5
Conclusion
A new study has shown that rosacea is a risk factor for malignancies, including basal cell carcinoma, squamous cell carcinoma, breast cancer, and melanoma. Furthermore, rosacea is associated with an increased risk of various comorbidities such as cardiovascular, gastrointestinal, neurologic, psychiatric, and autoimmune diseases. The interplay of genetic and environmental factors, involving cathelicidins, TRP channels, and mast cell activation, contributes to the pathogenesis of rosacea. As triggers exacerbate symptoms, understanding dietary and environmental influences is crucial. Managing rosacea poses challenges, requiring a multifaceted approach involving skincare, systemic and topical therapies, and individualised treatment plans.
References
- Thapa L, Xia J, Guo W, et al. Rosacea and Its Association With Malignancy: Systematic Review. JMIR Dermatology, 2023.
- Fischer GW, Travers JB, Rohan CA. Rosacea pathogenesis and therapeutics: current treatments and a look at future targets. Front Med, 2023.
- Paiva-Santos AC, Gonçalves T, Peixoto D, et al. Rosacea Topical Treatment and Care: From Traditional to New Drug Delivery Systems. Mol Pharm, 2023.
- Rivero AL, Whitfeld M. An update on the treatment of rosacea. Aust Prescr, 2018.
- Schaller M, Almeida LMC, Bewley A, et al. Rosacea treatment update: recommendations from the global ROSacea COnsensus (ROSCO) panel. British Journal of Dermatology, 2017.




